

Abstract
Background. The incidence of cancer in sickle cell disease (SCD) is of substantial interest since life expectancy of SCD patients has improved with 85-94%SCD patients surviving to adulthood1and the risk of cancer increases with advancing age. A limited number of case reports and surveys have suggested an increased risk of cancer in the SCD population. Two large population based studies have recently examined the incidence of cancer in the SCD population. Goldacre et al. reported an increased incidence of hematologic cancers and some solid tumors among 7512 SCD patients in England compared with patients hospitalized for minor medical and surgical conditions2. Wun et al. reported that compared to the general population, SCD patients had a 72% increased risk of hematologic malignancies and a 38% reduced risk of solid tumors3
Methods. We studied the incidence of cancer in SCD at the University of Illinois at Chicago (UIC) in a retrospective cohort study that identified SCD patients and cancer cases using ICD-9-CM codes. The study included SCD patients, all ages, seen at UIC between September 30, 2010 and September 30, 2015. An age, gender, race and ethnicity matched non-SCD cohort was selected from the general population of UIC patients from the same time frame. The incidence of cancer was compared between the SCD and non-SCD UIC patient cohorts. The study was approved by the Institutional Review Board. The data was provided by the University of Illinois Hospital and Health Sciences System Clinical Research Data Warehouse and stored in secure Redcap database.
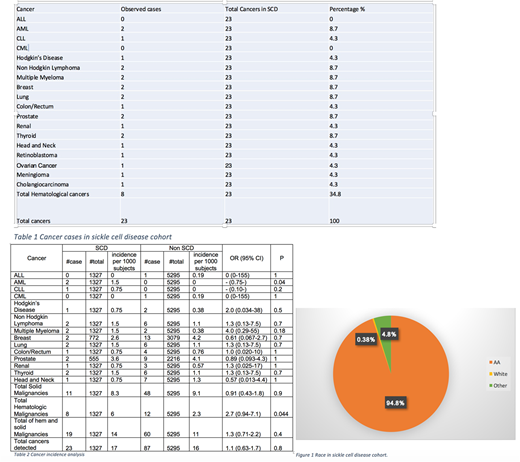
Results. There were 1327 patients in the SCD cohort, 41.8% males and 58.1% females. The breakdown by ethnicity was 94.8% African Americans (AA), 4.8 % other and 0.38% white patients as shown in Fig.1. There were 23 cancer cases identified in the SCD cohort (1.25%). The electronic medical records of all these cancers cases were reviewed to verify the cancer diagnosis. Amongst the cancer cases identified in SCD cohort there were 5 patients (22.7%) on hydroxyurea (HU) and 17 (77.3%) were not on HU. There were 8 (34.8%) hematological and 15 (65.2%) solid malignancies in the SCD Cohort as shown in Table1.There were 5295 patients in the control cohort, with breakdown by gender and race was identical to the SCD cohort. There were 87 cancer cases identified in this cohort (1.6%). There were 12 (13.8%) hematologic and 48 (55.2%) solid malignancies of the total cancers in control cohort. Fischer exact test was used to compare the cancer incidence in the SCD and control cohorts. Our study did not show statistically significant differences between the SCD and control cohorts for the incidence of total cancers (p=0.81) and solid tumors (p=0.87). There was increased incidence of AML and total hematological malignancies in SCD cohort and the difference was statistically different between SCD and control cohort (p=0.04) as shown in Table 2.
Discussion. To the best of our knowledge this is the only study where instead of relying on the registry and billing codes the SCD and cancer diagnosis was manually verified in the SCD cohort to maximally eliminate any inaccuracies in estimation of incidence. Goldacre et al. used hospitalization data in England and reported a threefold to 10-fold higher incidence of hematologic cancers among SCD patients and an increased risk for colon cancer, nonmelanoma skin cancer, kidney cancer, and thyroid cancer. Wun et al. reported increased risk of leukemia and low risk of solid cancers based on hospital admission and emergency department (ED) data, so healthier SCD patients, particularly children, may have been excluded. Our study data is not limited to inpatient and ED department and includes patients of all ages.
Our study shows that overall the cancer rates of those with sickle cell disease are not significantly different from the general population. There is increased incidence of hematological malignancies but the sample size is small. Nevertheless, due to treatment advances including hematopoietic stem cell transplant, increased awareness and better access to health care patients with SCD are living longer and there is a need to screen SCD patients for cancer just as vigilantly as for non-SCD patients.
Reference.
Maitra P,Ataga KI, Hematologica 102(4):626-636.(apr 2017)
Olena O Seminog, Michael J Goldacre, Journal of the Royal Society of Medicine; 2016, Vol. 109(8) 303-309
Ann Brunson,Ted Wun,Blood Volume 130 Number 13(September 2017)
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal